
Picture this.
It’s 1880 in the Old West. A gang of bandits lies belly-down in the sagebrush on a bluff overlooking a thriving town.
And its bank.
They have staked out the building, know its comings and goings, where the guards are positioned, and how to blow the safe. They are ready for the hold-up, but there is one more thing to do. Something that will ensure they not only get the money, but get away scot-free to enjoy it.
The rough, scarred gang leader, peering over his filthy bandana, eyes an accomplice and gives a definitive nod. The outlaw nods back, picks up a pair of pruners, and strolls to a collection of low-hanging cords snaking their way over the rocky crag of the bluff and trailing away into the desert landscape. The telegraph wires. The lifeline between remote outposts of the territory. The means of spreading news, exchanging gossip, and raising a posse. If a crime is committed, every lawman in the region will know within hours and be on the hunt.
The outlaw dons gloves, raises the blades, and – lop, lop – cuts the lines.
Isolation. Silence. The town is now alone.
The gang quickly rises up, mounts their horses, and lopes purposefully downward into the valley. The bank is theirs for the taking.
Unusual Care
Much of the time, medicine benefits from following definitive rules, established protocols, and predictable escalations in treatment. It is how patients are kept safe and the best outcomes are achieved.
This is often true in osteoarthritis (bony arthritis) therapy. Osteoarthritis is a frequent cause of joint pain worldwide. Although the exact mechanism is complex, a simple explanation is that cartilage loss leads to increased pressure on the joint, resulting in pain, swelling, and decreased function. Many treatments focus on reducing these symptoms through bracing, non-steroidal anti-inflammatory drugs (NSAIDs), steroid injections, or exercise therapy. If these interventions are ineffective, joint replacement is the definitive step.
But sometimes, treating difficult conditions requires approaching the problem differently. Thinking outside the box.
Behaving like an outlaw.
What does this look like in osteoarthritis treatment? Consider that we experience pain not just because a joint is damaged or injured but because something tells us it is so. Like telegraph lines, nerves send messages from a joint to the brain to describe its condition. The brain then interprets those messages as pain, heat, cold, soft, rough, or innumerable other sensations.
In the Old West, bandits would sometimes cut telegraph lines to disrupt communication. What if we did the same to nerves so the brain perceived pain differently, or not at all?
Radiofrequency nerve ablation works on this premise. It does not stop osteoarthritis, but it keeps pain signals from reaching the brain, greatly reducing discomfort and disability.
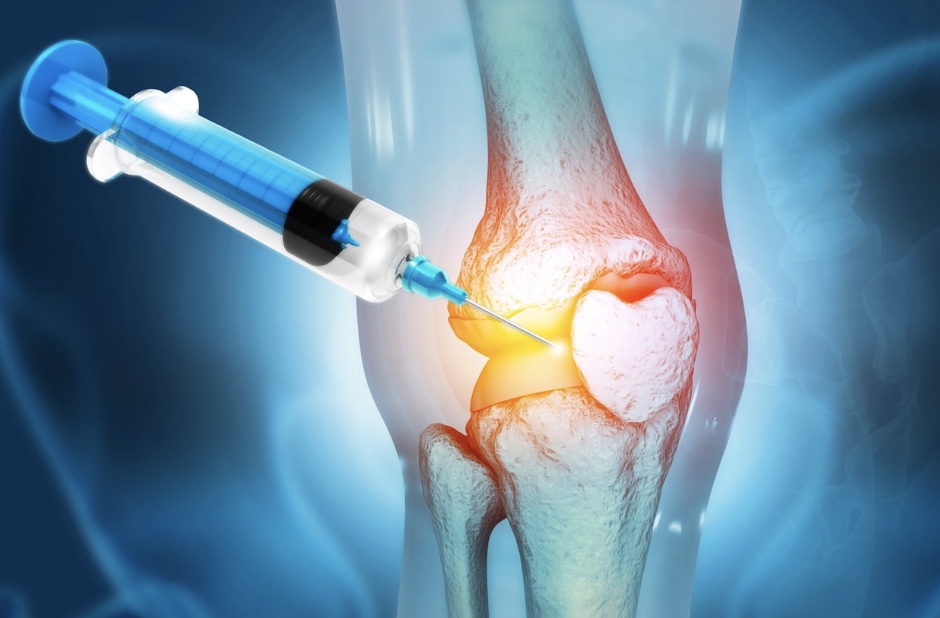
How is the Procedure Performed?
Radiofrequency nerve ablation is done by placing a needle with an electrically-heated tip close to a pain-sensing nerve. The exact location of placement differs with each joint. The needle burns the nerve so it does not transmit signals.
The nerves being treated are only used for pain, so numbness or weakness are not expected after the procedure. The ablation is not permanent; as soon as a nerve is burned, the body’s healing systems begin to repair it. Nerve ablation is intended to relieve pain for six to twenty-four months.
Nerve ablation consists of two steps: a diagnostic procedure and a therapeutic procedure. During the diagnostic procedure, the affected joint area is cleansed, and the skin is numbed with an anesthetic. Using either ultrasound or x-ray guidance, needles are placed close to the pain-signaling nerves, and a small amount of additional anesthetic is injected. The injection sites are covered with bandages, and the person being treated monitors his or her pain for a few hours afterwards. If pain is improved by 50% or better, it is believed nerve ablation will be helpful.
For the therapeutic procedure, a similar process is followed, except that special needles with heated tips are placed next to the nerve. Often, light sedation is used, similar to a colonoscopy. After numbing the area, the heated needle burns the nerve for 2-3 minutes. Following the procedure, a person is seen back in clinic in 2-4 weeks to make sure there are no complications.
Why Should I Consider Nerve Ablation?
One of the attractions of nerve ablation is that it is based on anatomy; the procedure interrupts known pain signaling pathways. Other benefits are that it is less invasive than joint replacement, provides long-lasting improvement, and is safe for those who cannot tolerate steroid injections or more invasive procedures. If a person can have a colonoscopy, they can have a nerve ablation.
Some considerations exist for nerve ablation. First, a person may need clearance from a general practitioner or cardiologist before proceeding. Second, some joint procedures may not be covered by insurance; consult both your healthcare team and insurance company for specific details.
In summary, radiofrequency nerve ablation is an effective treatment for pain and disability from osteoarthritis. It is minimally invasive, reduces discomfort, and is long-lasting. If a person has tried other conservative treatments without success or has medical reasons to avoid steroid injections or NSAIDs, nerve ablation is a very viable option.
References:
- Tran A, Reiter DA, Cruz AR, Gonzalez FM. Genicular Nerve Ablation Review Using Cooled-Radiofrequency Nerve Ablation. Semin Intervent Radiol. 2022 Jun 30;39(2):130-137.
- Soetjahjo B, Adriansyah D, Yudistira MB, Rahman AN, Herman H, Diwan S. The Analgesic Effectiveness of Genicular Nerve-targeted Cooled and Pulsed Radiofrequency Ablation for Osteoarthritis Knee Pain: A Systematic Review and Meta-analysis. Pain Physician. 2024 Sep;27(7):357-373.
- Nitz JN, Shiferaw BT, Bartley MJ, Moyer JR, Ruprecht KK, Matta AY, Abd-Elsayed A. Repeat Genicular Nerve Cooled Radiofrequency Ablation: Retained Efficacy or Diminishing Returns? J Clin Med. 2025 Jun 12;14(12):4194.






Leave a comment